Northwestern Medicine scientists have discovered a potent immunotherapy approach for treating meningiomas, the most common type of primary brain tumor, according to a recent study published in Nature Communications.
More than 39,000 Americans are diagnosed with meningioma each year, according to the National Brain Tumor Society. The tumor originates from cells in the meninges, a fibrous membrane that covers and protects the brain and spinal cord.
While some meningiomas can be treated effectively with surgery and radiation, more advanced and aggressive tumors are therapy-resistant and can recur with increased rates of morbidity or mortality.
“There are no systemic therapies shown to be consistently effective for meningiomas, and there is growing interest to use immunotherapies for targeting these tumors,” said Mark Youngblood, MD, PhD, a resident physician in neurological surgery and lead author of the study.
In the current study, the investigators sought to identify new immunotherapy targets for meningiomas by analyzing single-cell RNA sequencing datasets encompassing data from 22 patients diagnosed with meningioma tumors.
From this analysis, the scientists discovered that the STING pathway — which has been shown to play in a role in cancer by supporting anti-tumor immunity — is expressed both within the meningioma tumor cells and in the immune cells circulating within the tumor microenvironment.
“STING is actually expressed in the meningioma tumor cells themselves and not just in the infiltrative immune populations, which is unique from other types of brain tumors such as gliomas,” Youngblood said. “This provides an opportunity to target both immune and tumor cells directly in patients, and also represents a model to understand more about STING’s role in cell death.”
Next, the investigators administered an experimental drug that activates the STING pathway, called STING agonist 8803, in human meningioma tumor samples harvested directly from the OR. In previous work led by Heimberger, STING agonist 8803 was shown to reprogram previously suppressed immune responses in glioblastoma.
In the meningioma samples, the investigators found that 8803 inhibited tumor growth and promoted cytotoxicity of the tumor cells. This finding was duplicated in mouse models of meningioma, in addition to expected activation of latent immune populations. Notably, 8803 also reduced tumor volume and mortality in the mice.
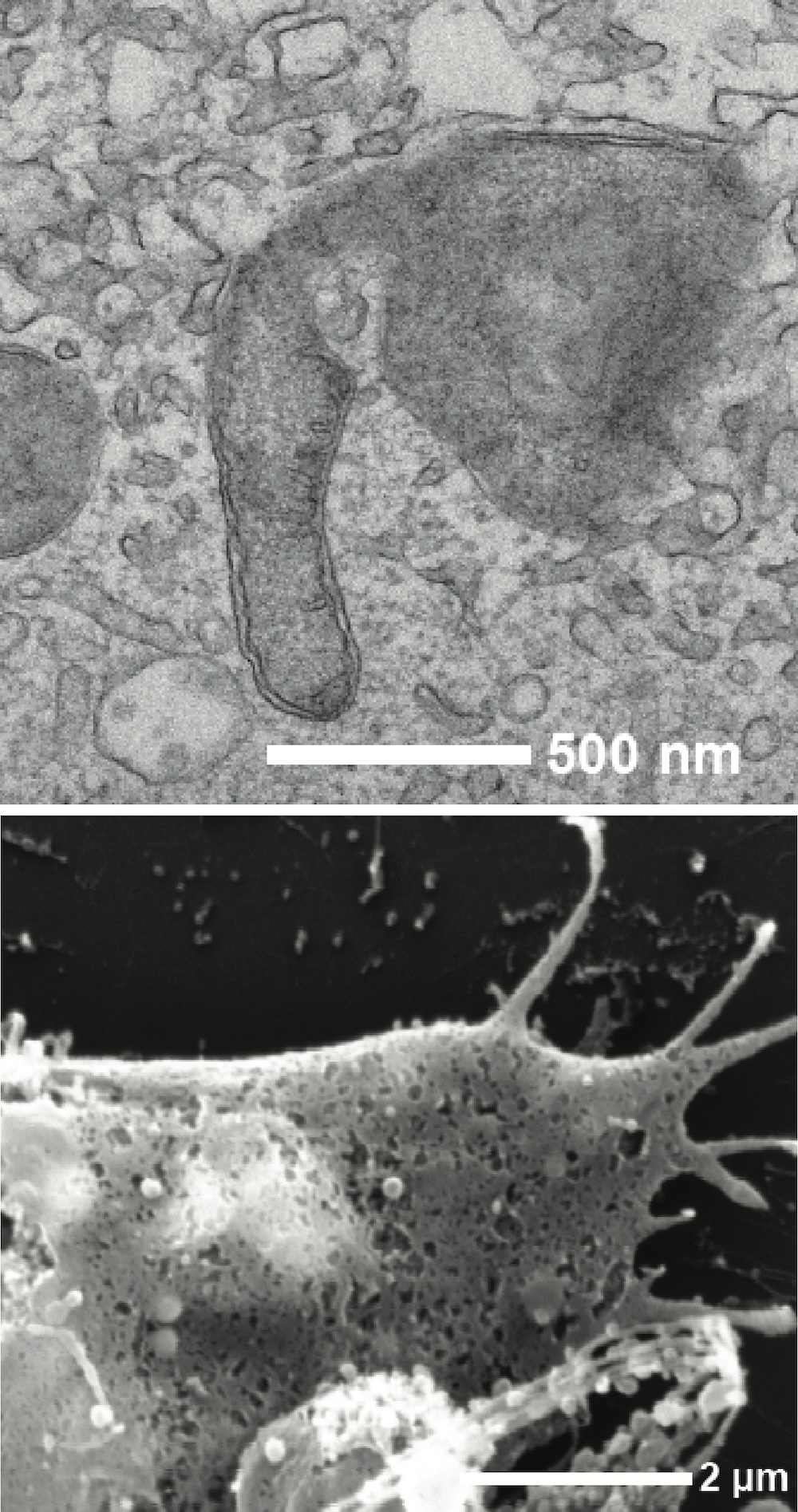
Lastly, to identify the cellular mechanisms promoting cytotoxicity in meningioma tumor cells, the scientists used RNA sequencing and electron microscopy to study meningioma tumor cells that had been treated with the STING agonist.
Unexpectedly, they discovered the drug triggers programmed necrosis pathways and activates the Gasdermin D protein, which in turn creates “pores” in the tumor cell membrane. Consequently, the lack of membrane integrity triggers an abrupt and uncontrolled form of cell death which releases antigens into the tumor microenvironment, causing an inflammatory response.
“It’s a very dirty type of cell death and, as a result, we think that it synergistically triggers even more immune activation,” Youngblood said.
Compared to other solid tumors, meningioma tumors harbor large amounts of collagen, which makes up much of the lesion’s bulk and can cause mass effect on the brain.
In meningiomas treated with the STING agonist, the scientists discovered that tumor cells showed a decrease in the production of collagen, while infiltrative immune populations increased the production of collagen-degrading enzymes, causing an overall reduction in the tumor mass.
“We’re hoping that in addition to arresting the growth of the tumor and causing the death of the tumor cells, we actually might see a lot of the bulk of the tumor reduced through this extracellular matrix degradation,” Youngblood said.
The findings highlight the widespread expression of the STING pathway in the meningioma tumor microenvironment and suggests that using STING agonist 8803 to target this pathway may be an effective approach for inducing direct tumor and inflammatory immune responses in meningioma, according to Youngblood.
“Outside of the potential clinical utility, this study is a great model for understanding more about how the STING pathway works, which has a lot of effects across many types of diseases even outside of cancer,” Youngblood said.
Amy Heimberger, MD, PhD, the Jean Malnati Miller Professor of Brain Tumor Research and vice chair for research in the Department of Neurological Surgery, was senior author of the study.
Co-authors of the study include Shashwat Tripathi, a student in the Medical Scientist Training Program (MSTP); Hinda Najem, MD, MS, a postdoctoral fellow in the Heimberger laboratory; Harrshavasan Congivaram, a third-year medical student; Mateo Gomez, a research assistant in the Youngblood lab; Caylee Silvers, a student in the Driskill Program in Life Sciences (DGP); Nishanth Sadagopan, a third-year medical student; Rahul Haliparambil, a third-year medical student; Ching Man Wai, PhD, research assistant professor of Biochemistry and Molecular Genetics; S. Joy Trybula, MD, clinical assistant professor of Neurological Surgery; Peng Zhang, PhD, assistant professor of Neurological Surgery; Jared T. Ahrendsen, MD, PhD, assistant professor of Pathology in the Division of Neuropathology; Pouya Jamshidi, MD, assistant professor of Pathology in the Division of Neuropathology; Daniel Brat, MD, PhD, the chair and Magerstadt Professor of Pathology; Rimas V Lukas, MD, associate professor of Neurology in the Division of Neuro-oncology; Roger Stupp, MD, the Paul C. Bucy Professor of Neurological Surgery and chief of Neuro-oncology in the Department of Neurology; Adam Sonabend, MD, assistant professor of Neurological Surgery; Maciej Lesniak, MD, the chair and Michael J. Marchese Professor of Neurosurgery; James Chandler, ’96 MD, ’96 GME, the Lavin/Fates Professor of Neurological Surgery; Matthew C. Tate, MD, PhD, associate professor of Neurological Surgery; Stephen Magill, MD, PhD, assistant professor of Neurological Surgery; and Jason Miska, PhD, assistant professor of Neurological Surgery.
This study was supported by National Institute of Health grants CA120813, NS120547, P30CA060553 and P50CA221747; the Remission Alliance; the Charlie Teo Foundation; Robert Mosky; the Malnati Brain Tumor Institute; the American Brain Tumor Association (fully supported by Tap Cancer Out); U.S. Department of Defense (CA230856); Neurosurgeon Scientist Training Program of the Society of Neurological Surgeons; and National Cancer Institute Training Grant T32 CA009560.