Using circulating tumor DNA to identify patients at risk of urothelial cancer relapse after surgical resection could help improve post-surgery treatment, according to a study published in Nature.
Patients who test positive for circulating tumor DNA (ctDNA) after surgery and who were treated with immunotherapy had improved disease-free survival compared to patients who were positive for ctDNA but did not receive immunotherapy. These results demonstrate the power of personalized medicine in cancer therapy, according to Maha Hussain, MBChB, the Genevieve E. Teuton Professor of Medicine in the Division of Hematology and Oncology and a co-author of the study.
“Better risk prediction allows for better individualized therapy intensification targeting micro-metastatic disease in patients who are at risk of relapse,” said Hussain, who is also deputy director of the Robert H. Lurie Comprehensive Cancer Center of Northwestern University.
Determining whether or not a patient has remaining micrometastatic disease after surgery with or without prior pre-operative neoadjuvant chemotherapy has been historically difficult, according to the authors. Many patients who are actually cured by surgery, with or without neoadjuvant chemotherapy, receive additional systemic therapy based on post-surgery pathology. Other patients with residual microscopic disease presence may not receive potentially beneficial treatment until disease progression has become detectable by imaging.
“Clearly, in oncology one size does not fit all,” Hussain said.
The presence of ctDNA is considered likely evidence of systemic disease and is increasingly used as a biomarker for cancer relapse in patients who’ve undergone surgical resection. Testing for ctDNA offers advantages in identifying patients with residual systemic micrometastasis, according to Hussain.
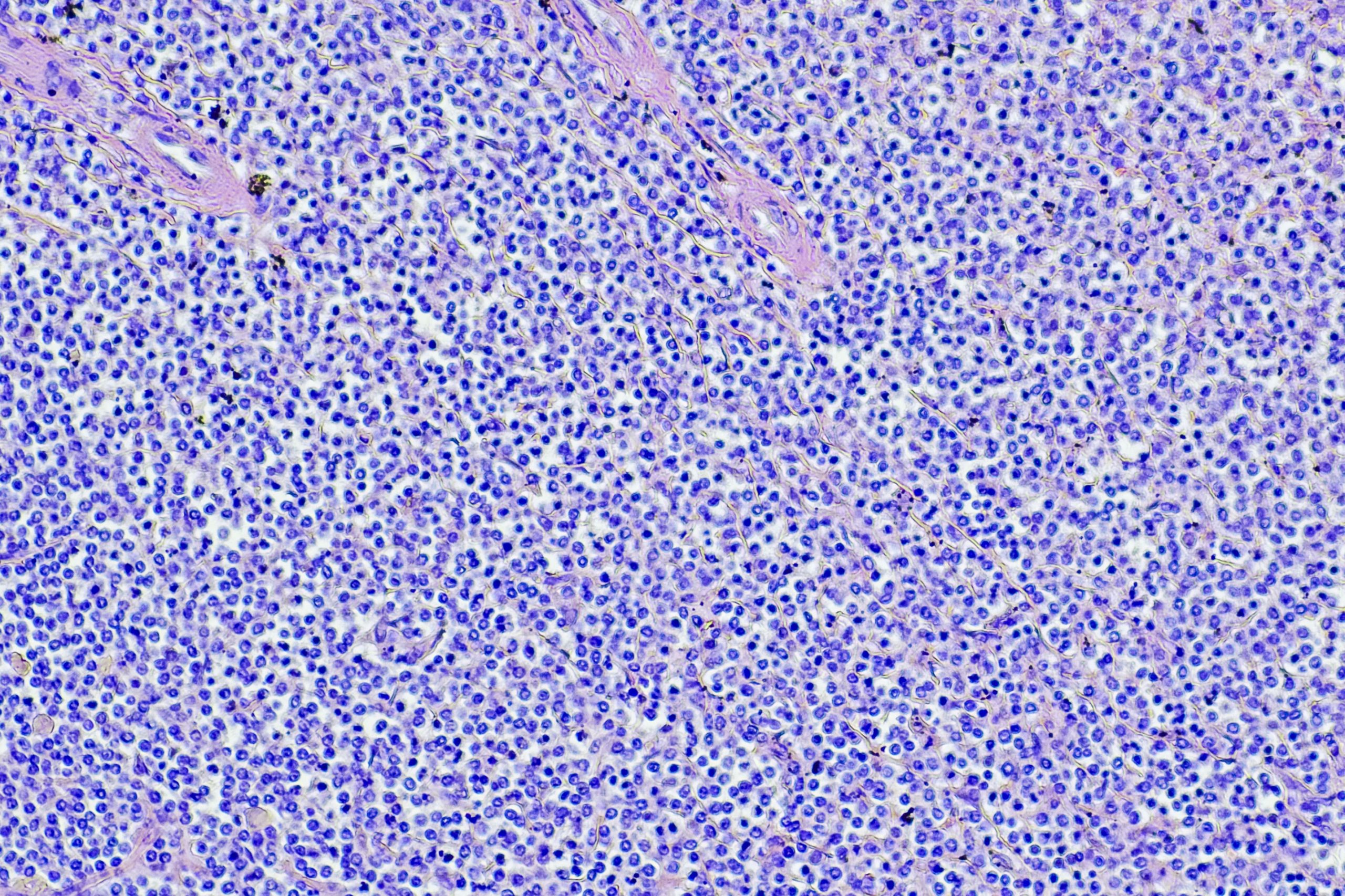
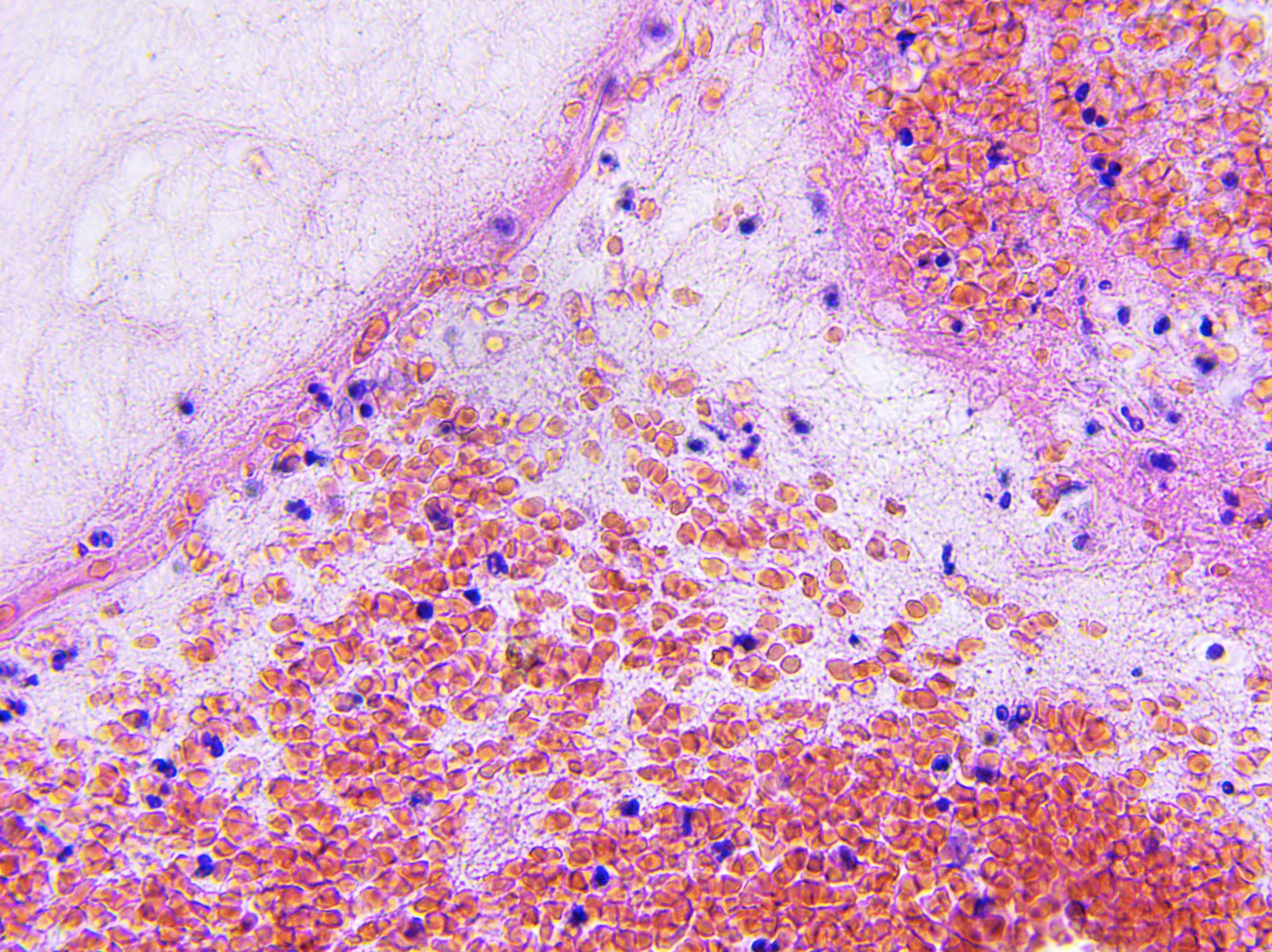
In the current study, investigators sequenced urothelial tumor cells and identified 16 tumor-specific mutations. If a patient sample showed evidence of two or more of these mutations, that patient was considered ctDNA-positive.
Patients were enrolled in a randomized study comparing outcomes for patients after surgical resection for urothelial cancer. One group of patients received atezolizumab, a PD-L1 immunotherapy, while the other group was simply observed after surgery.
While atezolizumab did not show a significant improvement in overall survival among all patients, those patients who were ctDNA-positive post-surgery and received atazolizumab did show improvement compared to similar patients who were ctDNA-positive but did who not receive the treatment. In fact, 18 percent of patients who were ctDNA-positive and received atezolizumab had their ctDNA completely cleared, a measure that was associated with improved outcomes.
This detection and treatment method does have limitations, according to the authors. Using ctDNA to detect cancer relapse only detected 60 percent of relapsed cancers in the observation group, likely a result of low ctDNA after resection of the primary tumor. While there is room for improvement on detection using ctDNA, this personalized approach could be a framework for post-surgical cancer care, according to Hussain.
“Better technologies in the future could further help these patients,” Hussain said.
The study was sponsored by F. Hoffmann-La Roche Ltd/Genentech.