

Patients undergoing radiotherapy for brain cancer often suffer cognitive decline after treatment, but a new method of delivering radiation could reduce the chance of those impairments, without compromising effectiveness, according to a new study published in the Journal of Clinical Oncology.
Called hippocampal avoidance (HA), this method reduces the amount of radiation delivered to the hippocampus; patients who were treated with HA methods had about a 25 percent fewer risk cognitive decline as compared to patients undergoing the standard treatment regimen.
“This is very important, as more of our patients are fortunately living longer with metastatic cancer, and therefore are at higher risks for developing brain metastases, and also may be at risk for long-term side effects of therapy,” said Timothy Kruser, MD, assistant professor of Radiation Oncology a member of the Robert H. Lurie Comprehensive Cancer Center, and a co-author of the study.
Vinai Gondi, MD, health system clinician in the Division of Radiation Oncology, was also a co-author of the study.
About 30 percent of patients with cancer will eventually develop metastases in the brain over the course of their disease. One current standard approach is whole brain radiotherapy (WBRT) combined with the neuro-protective drug memantine; nearly 200,000 patients receive the treatment every year.
While WBRT helps slow cancer progression and alleviates symptoms caused by growths in the brain, the therapy often comes with significant side effects: learning deficits, memory lapses and difficulties with spatial processing, according to the authors.
Recent studies have attempted to locate the source of this damage, and suggested the source was a subpopulation of neural stem cells located in the hippocampus. These stem cells are essential for learning and other cognitive functions, and are especially vulnerable to radiation damage, so the study authors devised a radiotherapy technique that would limit dosage to this region.
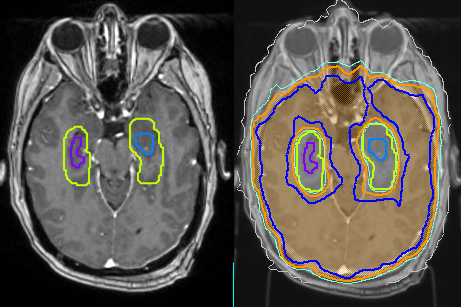
HA therapy works by measuring the hippocampus’ volume and location using MRI, and designing a radiotherapy pattern that contours around the hippocampus.
In the current study, investigators treated patients with either standard WBRT along with memantine, or HA along with memantine. After a median follow-up period of 8 months, the investigators found the risk of cognitive decline was significantly lower after HA therapy, when compared to standard WBRT.
Among the HA group, measures such as deterioration in executive function or learning and memory were nearly halved compared to the standard care group, and patients who received HA also reported less fatigue, less difficulty with remembering things and less difficulty speaking.
Importantly, there was no significant difference in survival between the two treatments, indicating that HA therapy doesn’t come with reduced effectiveness.
According to the authors, these results demonstrate that HA therapy should be the standard of care for patients with metastases outside the hippocampal region, and should be incorporated into future trials and treatments.
“This technique is readily available for use in radiation oncology clinics, and in conjunction with radiosurgery, gives radiation oncologists many tools to combat brain lesions while focusing on preserving memory and neurologic function,” Kruser said.
This study was supported by National Cancer Institute grants UG1CA189867 (National Cancer Institute Community Oncology Research Program) and U10CA180868 (NRG Oncology Operations).





