
Shifting machine learning workflows to a proactive model could speed data collection and analysis in healthcare, according to a viewpoint article published in JAMA.
Proactive models require less expert input, a boon in dynamic situations such as pandemics or in situations with many decision points such as chronic disease management, according to Yuan Luo, PhD, associate professor of Preventive Medicine in the Division of Health and Biomedical Informatics and lead author of the publication.

“There is more research that needs to be completed before we can make this transformation, but it could be applicable to many fields,” said Luo, who is also chief AI officer at the Northwestern Clinical and Translational Sciences (NUCATS) Institute and the Institute for Artificial Intelligence in Medicine, professor at the McCormick School of Engineering and a member of the Robert H. Lurie Comprehensive Cancer Center of Northwestern University.
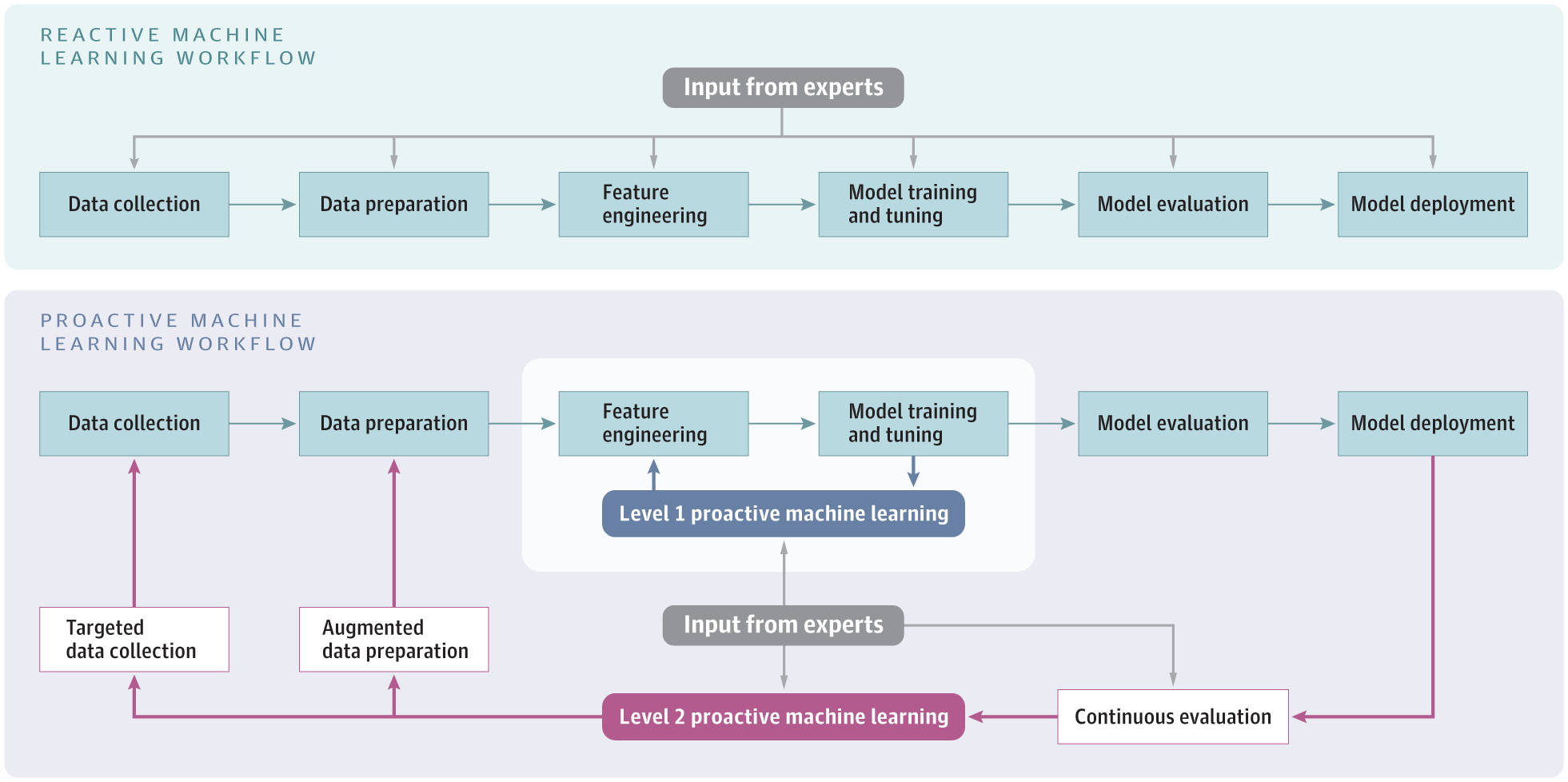
Machine learning (ML) algorithms are workflows that leverage statistical methods to glean useful patterns from data. In a conventional model, expert input is required at each step, from data collection to feature engineering and training, to eventual deployment and evaluation.
However, a proactive model automates some of these processes, such as evaluation to inform new data collection, Luo said.
“This can close the loop from deployment to data collection, refining data collection without expert input,” Luo said.
One notable example of proactive ML was used in Greece, helping target entry testing for travelers. The model, known as Eva, stratified travelers into risk categories using age, sex and travel history: a more accurate estimate of risk compared to merely using country of origin. This allowed Greek public health officials to allocate scarce PCR tests to maximize detection of infected travelers.
The proactive part of this model was the feedback; Eva automatically notified Greek officials which risk estimates were based on few or old data and needed to be updated, helping target new data collection that would eventually be rolled into the model.
“This told the human experts where they needed more data or if there was an emerging high-risk group, which can be useful in a rapidly changing pandemic,” Luo said.
Proactive ML models are still scarce overall, likely due to their complexity and unfamiliarity, Luo said, but could be useful in fields with a long time scale and many decision-points, such as chronic care management.
“This could help determine treatment regimen, and each decision would impact the model and help inform the next decision,” Luo said. “If you can model the complex situation faced by the patient, it could be a game-changer.”
Ultimately, these models need to make the jump from the virtual bench to the bedside, Luo said.
“It’s challenging for human experts to amass evidence and come up with insights as we are faced with growing data size and variety,” Luo said. “So we need to start deploying proactive ML systems into healthcare practice.”
Co-authors of the paper include Richard Wunderink, MD, professor of Medicine in the Division of Pulmonary and Critical Care, and Donald Lloyd-Jones, MD, ScM, chair and Eileen M. Foell Professor of Preventive Medicine.
Learn more about artificial intelligence in medicine at the Institute for Artificial Intelligence in Medicine.





