This article was originally published in the Breakthroughs Newsletter. Find more stories like this, as well as the Breakthroughs Podcast, on the Breakthroughs homepage.
As a student at the Royal College of Surgeons in Dublin, Ireland, there was a single thought on the mind of James Carr, MD, ’00 ’01 GME, chair and the Drs. Frederick John Bradd and William Kennedy Memorial Professor of Radiology.
“Because my father was a radiologist, I thought I was going to stay well clear of radiology,” said Carr.
He nearly pursued cardiology, but in the end, followed in his father’s footsteps, completing a radiology residency program at Saint Vincent’s Hospital (also in Dublin). Still, he held fast to his interest in the heart, focusing on the burgeoning field of cardiac imaging. This decision would lead him to Chicago for a fellowship in radiology, to a professorship at Northwestern and as of November 2018, to the chairmanship of the department.
Radiology holds a unique position within medicine. Radiologists primarily serve other physicians in the care of patients. This indirect clinical care approach puts a particular onus on collaboration, a philosophy that was instilled in Carr both through his training and through his father’s advice.
“One of the things I’ve learned is that we must work together across specialties to provide information that will help other physicians manage their patients better,” said Carr, who is also a professor of Medicine in the Division of General Internal Medicine and Geriatrics, and a professor of Biomedical Engineering at the McCormick School of Engineering.
Spending much of his career improving cardiac magnetic resonance imaging (MRI) to inform patient management, Carr knows that collaboration is essential to translate discoveries from bench to bedside.
“If you don’t have the interdisciplinary framework, the enterprise falls apart pretty quickly,” Carr said.
Translational Teamwork
Before a new imaging modality makes it to the clinic, physicists and clinicians must engage in an iterative process of optimization. What’s technologically possible may not be useful in the clinic, and functionality desired by doctors may be impossible for physicists and computer scientists to implement — requiring a continuous dialogue between MDs and PhDs, according to Michael Markl, MD, PhD, vice chair for research and the Lester B. and Frances T. Knight Professor of Cardiac Imaging in the Department of Radiology.
“You need the physics, engineering, and computer science background, but it needs to be tied to the expectations and experiences of clinicians,” said Markl, who’s also a professor of Biomedical Engineering at the McCormick School of Engineering.
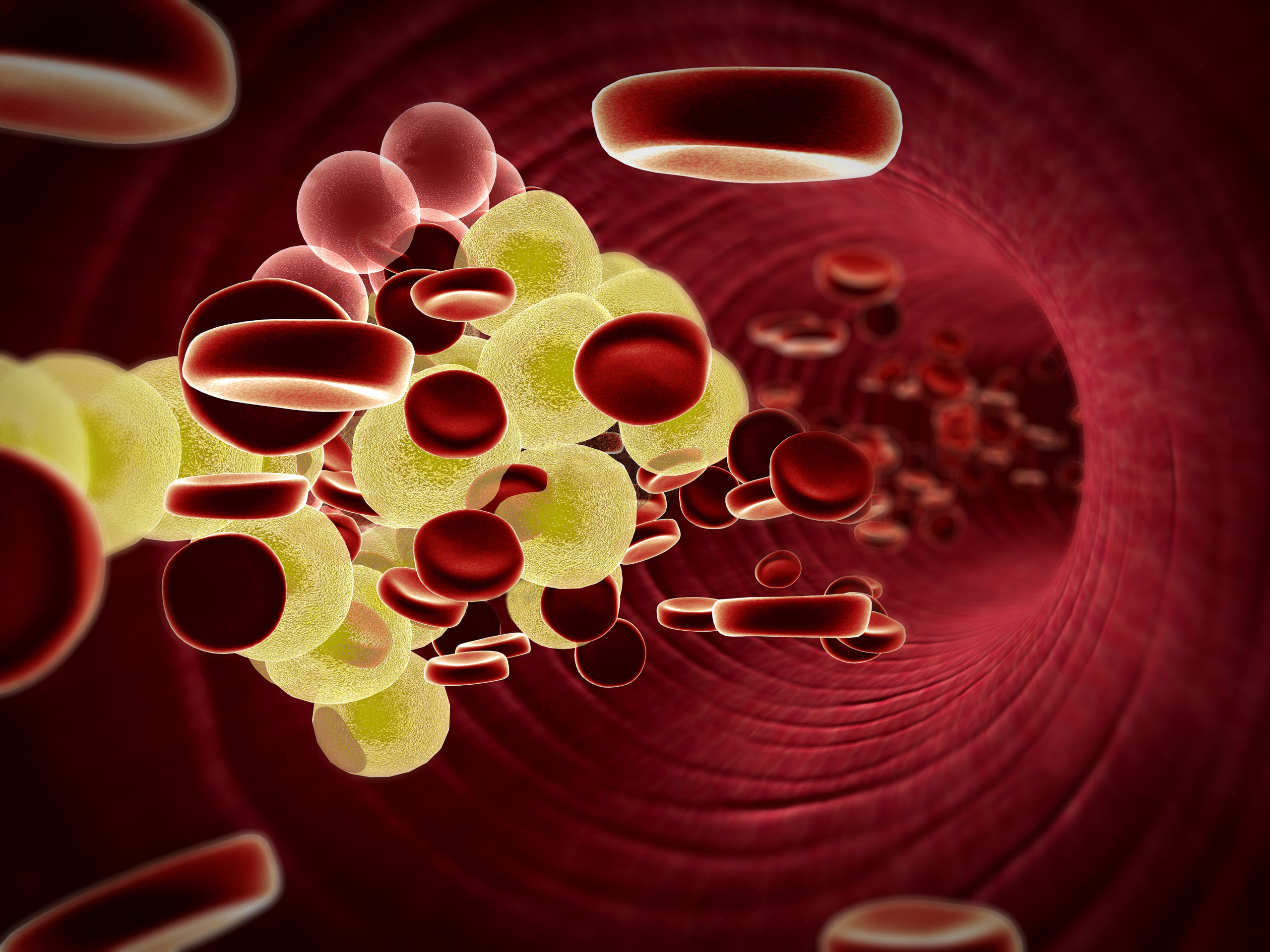
Feinberg has utilized this model to bring new imaging modalities and techniques to the clinic, such as a 4D flow MRI used to assess how blood flow is altered by congenital heart defects. Each individual’s heart has one-of-a-kind abnormalities, so understanding exactly how blood flows is invaluable for determining the course of care.
A decade ago, the scanning protocol for 4D flow MRI was long and arduous: The technique could only measure flow in a very small area of the heart, so it required a handful of different scans, each with its own precise patient positioning. Now, it requires just one scan, and much of the processing has been shifted after the scan — a big help for acquiring images from patients, particularly children, Markl explained.
“It helps to shorten scan time, because the child is often sedated or under general anesthesia because young children generally cannot tolerate MRI scans very well,” he said.
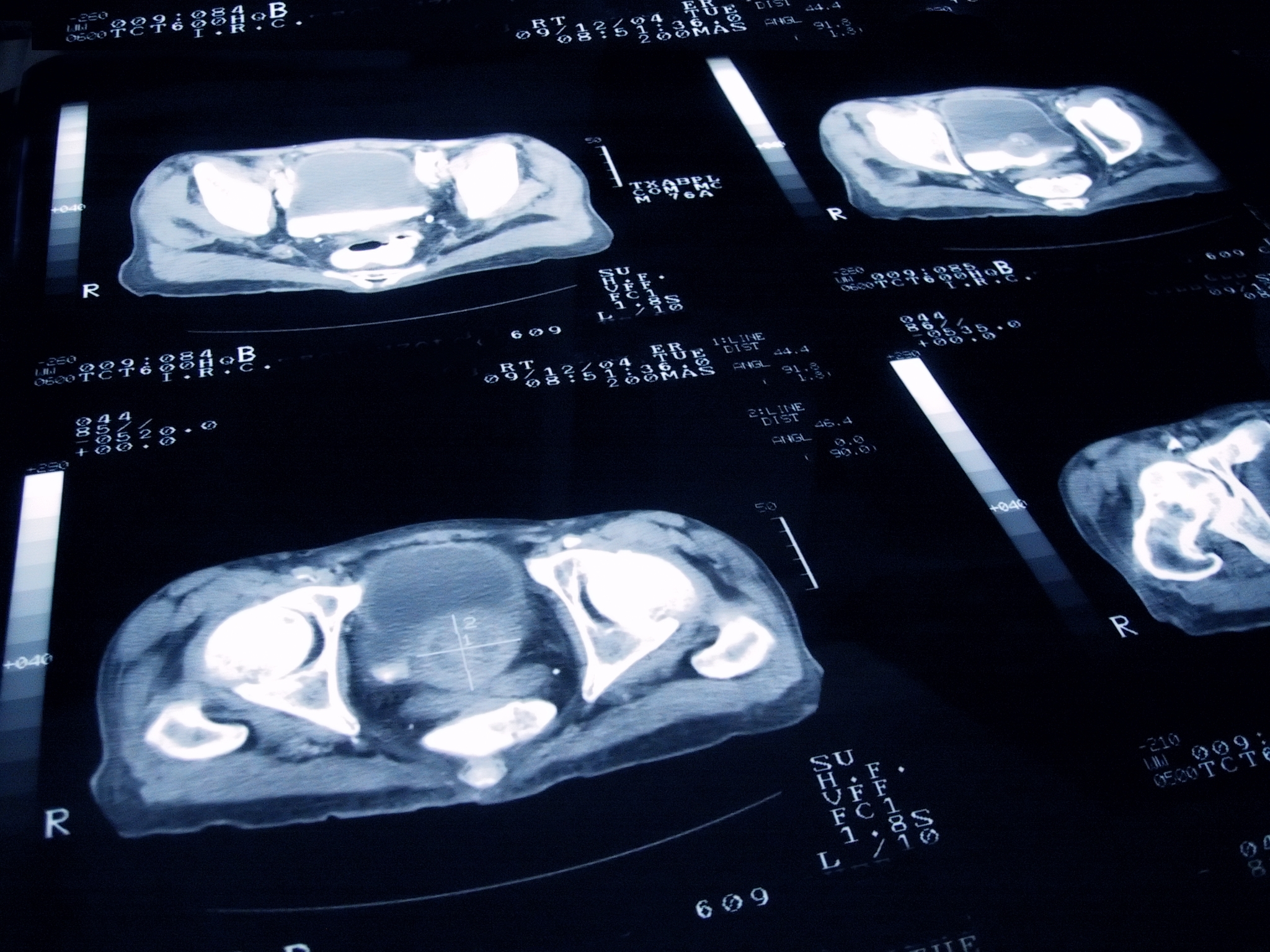
In addition, the processing and analysis step has been refined by Northwestern scientists. While a scan like an X-ray often produces just a handful of images, a single 4D flow MRI exam generates up to 10,000 images — many more than any radiologist can read in a reasonable amount of time. Northwestern scientists have built software to visualize that information, extracting numbers and parameters that are clinically relevant, Markl said.
Today, this exam is used weekly at the Ann & Robert H. Lurie Children’s Hospital of Chicago and Northwestern Memorial Hospital, a testament to the translational workflow that runs through every research project in the Department of Radiology.
“We have excellent partners in neurology, psychiatry, cardiac surgery, cardiology, Northwestern Memorial and Lurie Children’s,” Markl said. “It might seem like this at all academic medical centers, but it’s not — the opportunities for collaboration make Northwestern a unique place.”
Small Inventions, Big Impact
Radiology isn’t just diagnostic, either. The translational pipeline has also produced discoveries and actionable clinical improvements in treating liver cancer, for example.
One major issue with traditional chemotherapy is its side effects: In order to kill a tumor growing inside the body of patient, clinicians inevitably end up irradiating non-cancerous tissue. However, Northwestern scientists and clinicians have refined techniques to fight cancer from the inside, according to Riad Salem, MD, vice chair for Image Guided Therapy and chief of Vascular Interventional Radiology.
One innovative technique uses microspheres: microscopic glass beads with a radioactive core. In a technique called radioembolization, millions of microspheres are injected, through a catheter, directly to the liver.
“These are so small and once they become inert, they don’t affect anything — akin to sutures they might use in a surgery,” said Salem, who is also a professor of Medicine in the Division of Hematology and Oncology and a professor of Surgery in the Division of Organ Transplantation. “They emit their radiation for about two weeks and they’re very effective at killing the tumor. Our clinical outcomes are world-class and our research is redefining standards of care.”
These foundations put the department on strong footing for the future, which promises even more technological change and subsequent adaptation. Much has been made about the possibility of artificial intelligence (AI) replacing or crowding out the radiologist. In the near term, though, Carr sees AI as a way of augmenting physicians — rather than an existential threat — to handle the massive amounts of information that newer modalities can generate.
“It’s just not possible for a single human being to comprehend and understand all of that,” Carr said. “We need AI to help the radiologists do their job.”
Launching new AI research initiatives will pull from every discipline and challenge scientists, but Feinberg is uniquely positioned to be a leader in the budding science.
“Developing algorithms and partnering with our colleagues in Evanston and the larger industry will allow us to build a robust research program,” Carr said. “Because of our clinical volume and our digital infrastructure, we are poised to drive this whole area forward from a research perspective.”